
A 56-year-old Vancouver woman says she will die this month because British Columbia’s provincial government is refusing to cover essential health costs for her disabling illness.
“Madeline,” uses a pseudonym while advocating for herself because she and her health providers are concerned that the pressure of going public can compromise her health, and even kill her.
The main barriers preventing her from managing her symptoms and living with dignity is the lack of government support. She wants to live, but without coverage, her condition is deteriorating. Left with no other option, she’s been approved for medical assistance in dying (MAID).
She is one of 580,000 Canadians with a debilitating disease called myalgic encephalomyelitis (ME/CFS). According to researchers, the quality of life for people living with ME/CFS is substantially lower than those living with other diseases and conditions like lung cancer, depression, schizophrenia, multiple sclerosis, and rheumatoid arthritis.
Like more than 1.5 million disabled Canadians, she also lives in poverty. This number is likely to continue rising as more than 1.4 million Canadians infected with COVID-19 continue experiencing debilitating symptoms that are, in many cases, similar to ME/CFS.
The cost of severe forms of ME/CFS and long-COVID is substantial. The doctors who treat her condition have told her she must conserve her energy to live — that means receiving pre-made meals, housekeeping, and laundry services. The medicines, treatments, and other suggestions provided by medical professionals could cost upwards of $7,000 per month, she says. However, few of these services are subsidized, leaving Madeline reliant on the charity of medical care providers who perform discounted services.
“When I first started to deteriorate some 20 years ago, I made five attempts to get housekeeping, and I was refused [by the Ministry] every single time,” says Madeline, adding that her condition was considered an episodic illness. “To this day, I still can’t get housekeeping because there’s no category of coverage.”
Many people with ME and long-COVID experience a symptom called post-exertional malaise (PEM) due to these diseases breaking the body’s energy systems. “They have less energy to start with, use it up quicker, and recover slower. Repeatedly draining the battery can lead to less battery recharging and over time, less function and worsening symptoms,” says Jessica DeMars, a physiotherapist treating people with long COVID-19 at BreatheWell Physio.
“Conserving energy and pacing is considered, at the moment, the best management strategy.”
And while Madeline has been able to scrape by using money from a crowdfunding campaign for a few years, she has now run out of money.
She is one of a number of chronically ill people who have gone public in recent years to raise concerns about Canada’s expansion of MAID, questioning why the government has made it easier to access assisted death than the supports people with disabilities need to live.
Dr. Naheed Dosani, a palliative care physician, told Ricochet that people are choosing MAID out of desperation.

“We have seen in our public discourse many cases across Canada where people are thinking about and even pursuing MAID because they want to die because they’re not adequately being supported with the resources to live. This is concerning to me and should be concerning to every single Canadian,” he says.
In 2021, as the federal government moved to make MAID more accessible for patients, Dosani testified to the Canadian Senate, to share his experience providing street-based care for people with serious illnesses who also experience structural vulnerabilities like homelessness, poverty, and systemic racism.
He told senators that MAID can be arranged as quickly as two weeks, but it takes years to get people into housing, months to get income supports, and weeks to get mental health and harm reduction treatment, all of which are essential to a good quality of life.
“I found the whole thing morally distressing,” he says, describing why he asked to testify before the Senate. “If we are going to make it easier for people to get MAID, then we have a moral obligation to make sure they don’t pursue MAID because society doesn’t adequately support their needs.”
Out of funds, out of options
Recently, Madeline’s condition has deteriorated, which she says is the result of a lack of tangible support from the province, worsening symptoms she’s dealt with for over two decades, such as recurrent infections, extreme pain, exhaustion, and cognitive impairment.
“It’s really hard for me to be brutally honest about the measure of pain, exhaustion, and suffering,” she says.
Madeline was approved based on the low quality of life of the condition — directly caused by the lack of financial support. Her condition is manageable, but costly. Without additional coverage, she will deteriorate to death.
“MAID, for me, is not a life and death choice,” she says. “It’s about what kind of death I want when I run out of money.”
Without additional support, she says she will die imminently. She doesn’t have to schedule a time to die in advance, but when she feels her condition deteriorates enough, she can call up her assessors to set up an appointment.
“I shouldn’t be at the mercy of charitable support,” she says.
Madeline lives alone in her Vancouver, B.C. apartment, subsiding on the $1,483.50 in disability payments from the province. Until August, only $375 of this allowance can go to pay rent, based on a shelter allowance policy established in 2007 when the average rent for a two-bedroom apartment was about $900. Now, new legislation has increased this allowance to $500, even though the average cost of rent has roughly tripled. She turned to crowdfunding, but it hasn’t been enough to manage her condition.
There’s $5,040 worth of expenses for physiotherapists and other medical specialties like massage therapy. However, the province only covers $23 per visit for 10 visits yearly. She spends around $350 monthly on pharmacy items to manage symptoms, though the clinic recommends a regimen of $470 per month. Another $560 a month on supplements, though she would need to spend closer to $800 to get all of the supplements she needs. Then there’s another $700 for a pre-made specialized meal for her celiac disease. The Ministry only provides $45 monthly for general vitamins and minerals, and $180 monthly for other dietary needs.
Proper housekeeping costs close to $400 to $800 per month, though she cannot afford it. There is no allowance for these services. And up to $400 monthly for medical transport to her appointments. The Ministry only covers $0.36 per kilometer.
Altogether, that’s about $5,000 for essential medical services she needs at the bare minimum to live. However, in factoring in recommendations from the complex chronic illness clinic she visits, she would need to spend closer to $7,810 monthly. That comes to $93,720 annually, which isn’t unusual for many people with disabilities.
“I found treatments, but I can’t afford them,” she said.
Living within the constraints of provincial aid is near impossible
Getting any type of disability aid or coverage involves heaps of confusing paperwork — Madeline recalls that neither she nor her doctor could complete parts of the application.
“I brought one of those forms to my legislative office, and one of the staffers, a lawyer, looked at the form and said she didn’t know how to [fill it out],” says Madeline. Her disability advocate, Helaine Boyd, at the Disability Alliance BC (DABC), has been helping her with paperwork.
“It can be quite degrading for a person to have to prove their disability and to show all of their bank accounts,” Boyd said. “You really have to show that you have no other recourse, and then once you are on disability, assistance is extremely punitive.” She says that there are many ways that the province can claw back the amount of disability assistance that people like Madeline receive.
Sharareh Saremi, the advocacy access program manager for the DABC, which provides legal resources and support to persons applying for disability payments in the province, says that’s especially challenging for people who have any kind of cognitive restrictions. “There are a lot of hoops to jump through, and two steps to applying (financial qualification and disability qualification) which makes.”
The complexity means that some get rejected because of incorrect or inefficient information.
Not getting disability support can be devastating for patients who often need help with laundry and housekeeping, services that are often outside of what they can afford. This helps patients save their energy for the things that help ease their symptoms, bring them joy, and give them a better quality of life.
“We wouldn’t expect someone with ALS, severe MS, or other severe chronic disease to have to do these things — and likely there would be support available,” said Demars. “Unfortunately ME is poorly understood and comes with stigma, which leaves people without any support.”
Everyday challenges
“I’ll often wake up at 1 a.m. or 4 a.m. and I’m unable to get back to sleep,” Madeline said. “I have to strategize waking up and taking the first meds of the day.” Every day comes down to these tradeoffs that most of us don’t need to make or even consider. Even going to the bathroom takes effort and energy.
She has to figure out when she should take medications and how that will impact what she can and cannot eat. Pre-made store meals that fit her dietary restrictions aren’t always healthy. If she goes out for an appointment, she has to ensure she has energy. On average, she may have three to five appointments in the week.
Before leaving for an appointment, getting ready and out the door will take her up to six hours. The first few hours of the day are spent waiting for her supplements and medications to kick in. “If I’m able to take my mobility scooter to the appointment, then I have to strategize the flattest routes because most of the sidewalks are a hellscape of cracks and lifted slabs of concrete.”
Through careful planning and energy preservation, she can do some of the activities she is passionate about — enjoying time with friends, gardening, and volunteer events in the community. However, with her recent deterioration, she has been forced to spend more time in bed.
Death by poverty?
Due to a lack of resources and support, Madeline may deteriorate to a point where she can’t eat or speak.
According to the Canadian Association of MAID Assessors and Providers, which educates and trains medical providers to perform this procedure, poverty isn’t a sufficient reason for MAID.
Ricochet reached out to CAMAP for comment, but the office declined an interview. However, president Dr. Stephanie Green sent Ricochet a statement saying the organization doesn’t support any patient’s request for MAID based primarily on economic need. However, that may contradict information provided by other members of the organization.
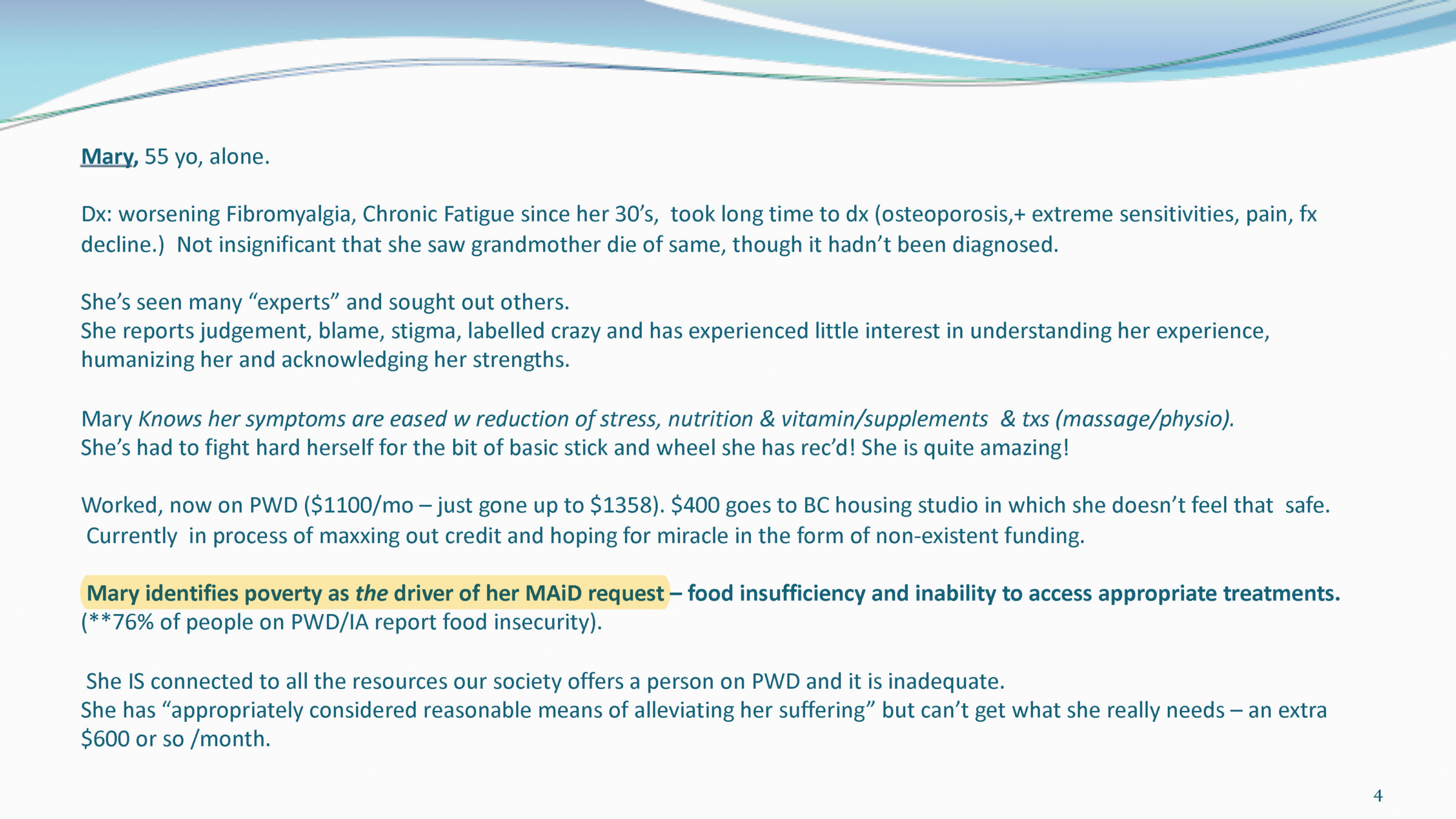
In videos obtained by the New Atlantis that teach trainees how to assess MAID eligibility, some experts teach that poverty is a defensible rationale for MAID. During a 2021 CAMAP seminar, presenters describe a case where poverty is the driver of a woman’s MAID request due to inadequate access to housing, medicine, and other resources. “Mary does not want to die, but she’s suffering terribly and she’s been maxing out her credit cards. She has no other options.” In another case, a woman who is no longer able to work, applies for MAID because of an inability to find affordable housing.
Mark Johnson, a spokesperson for Health Canada and the Public Health Agency of Canada, said CAMAP and Health Canada do not draw the link between disability, poverty, and MAID, which many experts, advocates, and disabled people have highlighted is increasingly pushing people to request euthanasia.
The reality is, while people may not be approved for MAID because they live in poverty, living in poverty deteriorates their health to the point that they qualify.
Dosani told Ricochet it is very difficult to distinguish the suffering caused by an illness, disability, or other medical condition from poverty and other social determinants of health. “People who experience social disparities don’t have a choice to be able to live well because they don’t have access to the resources they need.”
Madeline explained that anyone living on disability support payments alone will absolutely deteriorate because they cannot afford food, housing, and other resources to manage their condition.
The Canadian MAID regime is lacking the safeguards, data collection, and oversight necessary “to protect Canadians against premature death,” writes Cambridge University Press.
Dosani says the system is failing the most vulnerable. “We are on a difficult ethical journey. Is it really a choice when people don’t have the resources they need to live well?
“I’m worried our elected officials have made it easier to die with dignity than live with dignity through access to housing, income, food security and medication coverage. We should really think about what they says about us as a society.”
While the majority of people who qualify for MAID have a foreseeable natural death due to cancer or other conditions, people like Madeline can qualify due to debilitating conditions. The most recent federal report states that 10,064 people received MAID in 2021 — 219 of which did not have a foreseeable natural death.
At the end of the report, it details new regulations for monitoring MAID that would increase data collection to “improve our understanding of the socio-economic circumstances of MAID recipients.” However in the entirety of the 47 page report, it does not mention “poverty” at all.
“It is very important that different levels of government work closely together and collaborate to ensure that the appropriate data is collected to provide important safeguards to protect vulnerable populations,” Dosani said. “It is crucial for public safety and public confidence in the implementation of medical assistance and dying that we’ve got this data made available.”
Now, the federal government is considering expanding MAID again to include those suffering exclusively from mental illness, a move that was previously delayed by one year. That change is expected in March 2024.
28% of survey respondents think “homelessness” is a sufficient reason to pursue MAID. Homelessness has medical outcomes, but it is not a medical condition; it’s a condition created by societies that withhold vital resources. People need care, not death. https://t.co/0YqdQ9tpd0
— Diana Chan McNally (@Diana_C_McNally) May 17, 2023
Gabrielle Peters, a B.C.-based disabled writer, and policy analyst, who testified to the Canadian Senate on how MAID will impact working class disabled people. She says the way the Canadian government has implemented MAID is deeply unethical. “I do not believe that MAID can ever be made safe in this society,” she says. “MAID is a policy that creates a legal exemption for killing.”
The Ministry of Social Development and Poverty Reduction, which assesses disability applications in the province, declined to answer questions or provide any data regarding disability payments or supplemental services provided, nor any information as to which populations are applying for MAID and why.
Madeline says the Ministers of Health and Finance in B.C. are aware of her issues, and she’s been told that the Premier is also aware of her situation.
Both the federal Ministry of Health and B.C.’s Ministry of Health declined Ricochet’s interview requests and refused to provide any further information.
“We don’t really know the full magnitude of the problem because we don’t have the robust set of data we need to to fully understand the situation,” Dosani added. If this data was made publicly available, it would make it possible to answer whether people living with disabilities or other medical conditions, fall through the cracks, and end up applying for MAID.”
Madeline says that whenever she contacts the Ministry, it’s an exhausting experience, which is not something someone in her condition should have to deal with. “It isn’t helpful if you don’t have money because nothing they suggest is covered by the Ministry.”
With more than a million disabled Canadians living in poverty, Madeline hopes change is coming soon. She wants to see the government increase disability payments, so they are liveable while increasing funding for ME and other chronic conditions.
“Despite saying they wanted to support the most vulnerable, the federal government’s actions and lack of financial support during the pandemic felt like a kick in the head,” she says.
“The government is able to provide for these needs. The government is, however, unwilling,” she says.
When her condition inevitably deteriorates even more, she can reach out to the assessors who can arrange her procedure in her home, an office, or a hospital setting.
Without improvements in disability coverage within the province, Madeline will die of a manageable condition because she could not afford the treatment.
Madeline is a pseudonym used to protect anonymity. Her identity has been verified through her disability advocate. If you’d like, you can donate to her crowdfunding campaign and learn more about her through her podcast.
With files from Andrea Houston




{kind=link}